Can station-specific lymph-node metastasis risk be estimated before surgery?
Develop and validate models that combine tumor location, clinical staging, histology, and registry outcomes to support KLASS-standardized surgical planning.
이 포트폴리오는 이혁준 교수님의 지도 아래 서울대학교병원에서의 박사과정 연구를 위해 준비되었습니다.
Physician · University of Heidelberg
I want to validate station-specific lymph-node metastasis risk guidance for KLASS-standardized gastrectomy — using AI tools I have already begun building as independent proof-of-concept projects.
A 58-year-old patient undergoing robotic gastrectomy. Preoperative imaging suggests possible station 12a involvement, but intraoperative visualization is ambiguous.
A surgeon relying on experience might skip the dissection to avoid hepatic artery injury (under-treatment) or pursue it aggressively at elevated risk of morbidity.
A calibrated decision-support system could overlay a probability estimate — e.g., "Station 12a: 35% metastasis risk based on tumor characteristics and visual features" — converting intuition into quantified data that can be validated against outcomes.
The KLASS framework provides standardized procedures, quality metrics, and prospective registries — the ideal environment to close the gap between AI capability and clinical utility.
Each project addresses one component of the proposed PhD. They are independent building blocks on public data — not an integrated system.
Can published station-level prevalence be turned into a transparent surgical decision-support prototype?
Interactive descriptive prototype for 11 perigastric stations using systematic-review T-stage prevalence as the professor-facing evidence layer; individualized calibration is future work.
Literature-informed scaffold; calibration pending
⚠ All values are placeholders — not validated for clinical use. Real validation requires SNUH/KLASS registry data.
Can a surgical-video segmentation pipeline move from laparoscopic benchmark data toward robotic gastrectomy instrumentation?
Validated leave-videos-out CholecSeg8k benchmark work, a public gastrectomy domain-shift demo, and a preliminary SISVSE transfer-learning run using public robotic distal-gastrectomy frames.
CholecSeg8k CV: mean IoU 0.7574 · Dice 0.8614 (DeepLabV3; U-Net vs DeepLabV3 difference not statistically significant, p≈0.21) | SISVSE Run B: zero-shot IoU 0.0642 → fine-tuned IoU 0.4913
⚠ Preliminary public-dataset evidence only — not a validated clinical model, not trained on private SNUH data, and not suitable for clinical use.
| Evidence | Dataset / source | What it shows |
|---|---|---|
| 5-fold leave-videos-out CV | CholecSeg8k · 8,080 annotated frames / 17 videos | Reproducible benchmark proof-of-method for laparoscopic instrument segmentation |
| Public gastrectomy clip demo | PMC3752361 · 150 sampled frames | Qualitative domain-shift check on public laparoscopic gastrectomy footage |
| SISVSE Run B transfer | Public SISVSE robotic distal-gastrectomy frames · N=480 test frames | Zero-shot transfer was poor; targeted SISVSE fine-tuning substantially improved segmentation |
| SISVSE setup | Macro IoU | Macro Dice | N | Interpretation |
|---|---|---|---|---|
| Zero-shot CholecSeg8k → SISVSE | 0.0642 | 0.1148 | 480 | Strong laparoscopic→robotic domain gap |
| Fine-tuned on SISVSE | 0.4913 | 0.6260 | 480 | Preliminary transfer signal after target-domain adaptation |
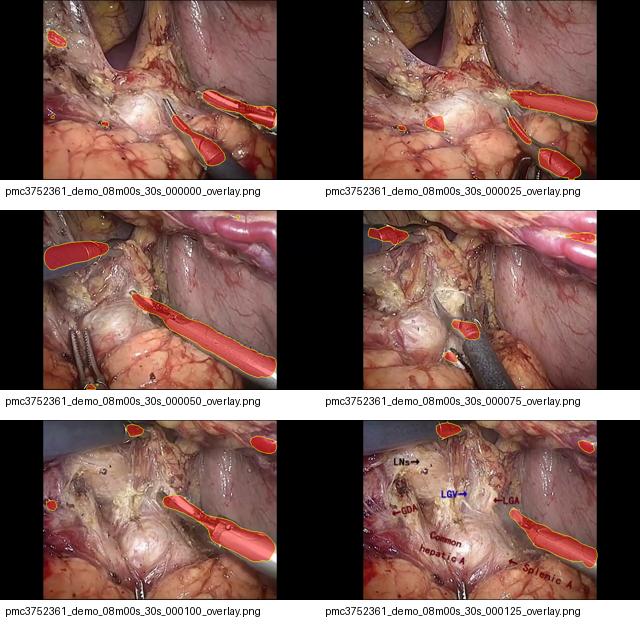
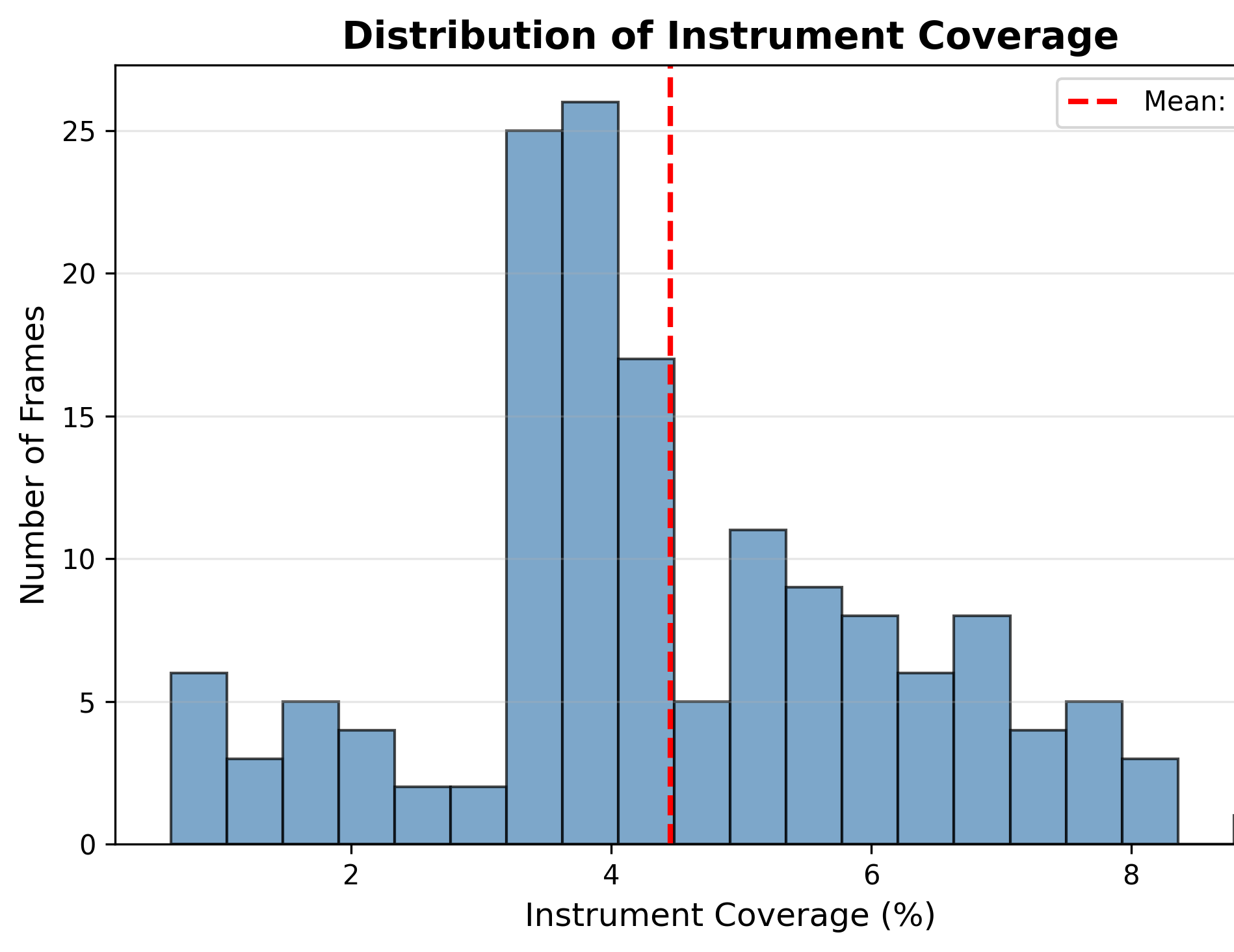
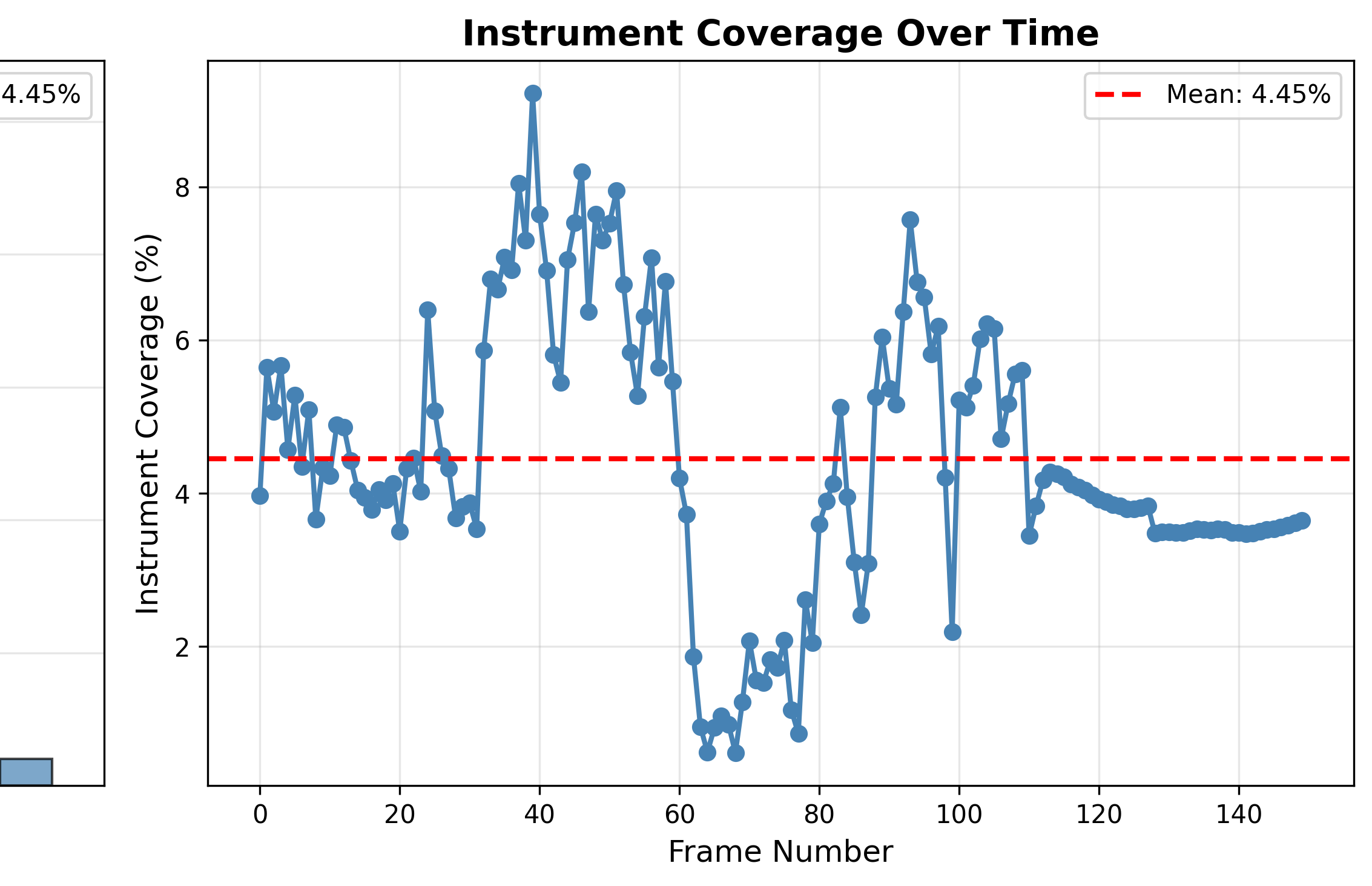
Representative public-dataset examples: one success, one typical case, and one failure case. Included deliberately to show both capability and limits.
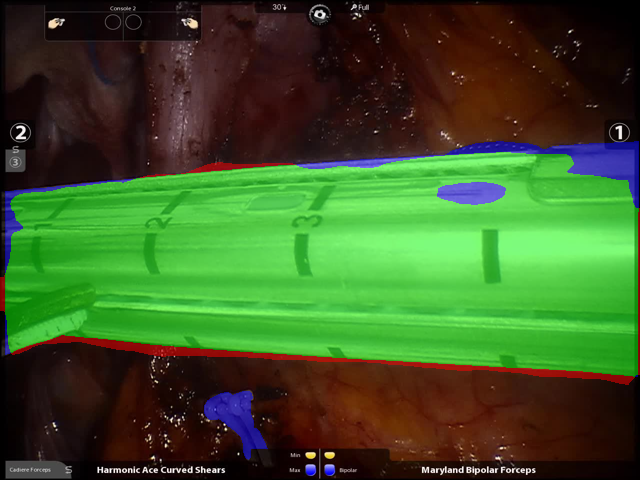
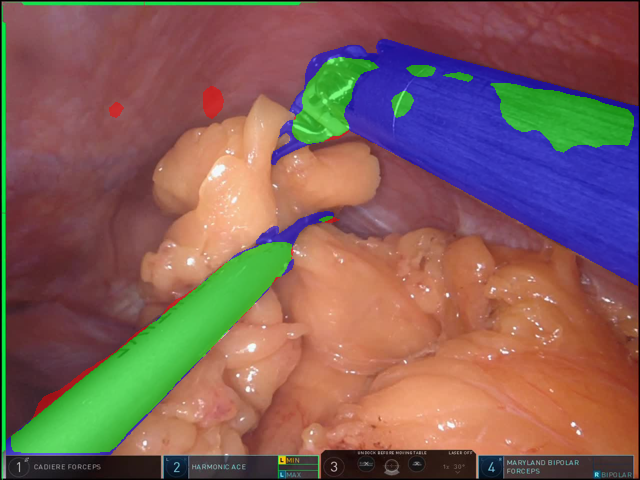

The SISVSE result is intentionally framed as preliminary public-dataset transfer evidence: zero-shot transfer from CholecSeg8k to robotic gastrectomy frames failed badly (macro IoU 0.0642), while target-domain fine-tuning improved macro IoU to 0.4913 and macro Dice to 0.6260 on 480 held-out frames. This supports the feasibility of the technical workflow, but clinical validation would still require permissioned SNUH robotic gastrectomy data, IRB/privacy review, and prospective evaluation.
How do we ensure AI predictions are clinically trustworthy, not just accurate?
Implementation of validation methodology principles inspired by TRIPOD/PROBAST: discrimination (C-index), calibration (Brier score, ECE), and survival analysis linkage (Cox regression, Kaplan-Meier). Decision-curve analysis is planned but not yet implemented.
Survival analysis pipeline tested on TCGA STAD; prediction and calibration models demonstrated on synthetic data
⚠ Demonstrates validation methodology, not novel algorithms. Clinical validation requires prospective SNUH data.
| Dimension | Metric | Purpose |
|---|---|---|
| Discrimination | C-index | Does the model rank patients correctly? |
| Calibration | Brier, ECE | Are predicted probabilities accurate? |
| Clinical utility | Decision curves (planned) | Does using the model improve decisions? |
Validation methodology inspired by TRIPOD/PROBAST principles — not novel methods, but rigorous application to surgical AI. Decision-curve analysis is planned for future work.
What is the survival landscape across gastric cancer stages?
Reproducible pipeline generating TNM heatmaps, Kaplan-Meier curves, and stage distributions from TCGA STAD PanCanAtlas data, with Benjamini-Hochberg correction for multiple comparisons.
6-fold survival differential documented (Stage IA: 72.2 mo vs Stage IV: 12.0 mo)
⚠ Based on public TCGA data — KLASS registry data needed for clinical applicability.
Median overall survival by AJCC stage (TCGA-STAD, n≥15 per stage). Omnibus log-rank χ²=33.09, p<0.001 (Benjamini-Hochberg corrected). "Not reached" = median beyond follow-up.
How do nodal status and surgical quality (lymph-node yield) shift recurrence risk?
Dual-model demonstrator: a KLASS-inspired logistic recurrence model alongside the Han 2012 D2-gastrectomy survival nomogram, with a lymph-node-yield sensitivity analysis illustrating the impact of nodal yield on recurrence risk estimation.
Educational demo on TCGA STAD (n=436) · model-estimated 5-yr survival ~91% (T1N0) to ~52% (T4N3)
⚠ Educational demonstration — coefficients are pedagogical approximations, NOT a validated clinical calculator (the Brier score of 0.502 reflects an endpoint mismatch, not accuracy).
Assumes age 58 and stage-typical tumour size (per repository imputation). Increasing examined nodes lowers the positive-node ratio → lower estimated risk, demonstrating why adequate D2 lymphadenectomy matters for accurate staging.
This professor-facing mode uses published T-stage prevalence across 11 perigastric lymph-node stations and keeps the other modifiers visible only as future work.
Canonical provenance and descriptive evidence layer: the-station-risk-map. Source table: systematic review PMC9852106.
Professor-facing mode: only T stage changes the displayed percentages. Location, size, and histology controls are shown for demonstration of future capabilities — they do not affect the current prevalence values.
Use this to reproduce a screenshot setup for the one-pager or research statement.
Descriptive literature prevalence only — not individualized prediction or clinical guidance.
Develop and validate models that combine tumor location, clinical staging, histology, and registry outcomes to support KLASS-standardized surgical planning.
Extract anatomy, exposure, and surgical-quality signals from gastrectomy video and test whether they add clinically meaningful information beyond preoperative variables.
Use SISVSE as public preliminary transfer evidence, then evaluate on permissioned SNUH robotic gastrectomy footage only after IRB/privacy approval and proper data governance.
IRB approval, data governance setup, video capture protocols. Build baseline station-specific risk models from KLASS registry data (Aim 1). Pre-register all inferential analyses. Target: 60–80 prospective cases.
Integrate intraoperative visual features with preoperative risk factors. Quality metric extraction and reliability validation (Aim 2). Feasibility study with 60 prospective cases. Target: 150–200 total cases.
Rigorous internal validation with subgroup analyses. Multimodal fusion pilot if Aims 1–2 on track (Aim 3, exploratory). Complete dissertation. Drafted multicenter protocol for post-doctoral work.
This research requires high-volume standardized gastrectomy, mature prospective registries, established quality metrics, and active surgical technology research. No other environment combines these elements for rigorous AI validation.
Downloads